Primary neurocritical care involving therapeutic hypothermia for acute ischemic stroke patients with malignant infarct cores
Article information

Abstract
Background
Acute ischemic stroke patients with malignant infarct cores were primarily treated with neurocritical care based on reperfusion and hypothermia. We evaluated the predictors for malignant progression and functional outcomes.
Methods
From January 2010 to March 2015 ischemic stroke patients with large vessel occlusion of the anterior circulation with infarct volume >82 mL on baseline diffusion weighted image (DWI) within 6 hours from onset, with National Institutes of Health Stroke Scale ≥15 were included. All patients were managed with intent for reperfusion and neurocritical care. Malignant progression was defined as clinical signs of progressive herniation. Predictive factors for malignant progression and outcomes of decompressive hemicraniectomy (DHC) were evaluated.
Results
In total, 49 patients were included in the study. Among them, 33 (67.3%) could be managed with neurocritical care and malignant progression was observed in the remainder. Decompressive surgery was performed in nine patients (18.4%). Factors predictive of malignant progression were initial DWI volumes (odds ratio [OR], 1.01; 95% confidence interval [CI], 1.00 to 1.02; P=0.046) and parenchymal hematoma (OR, 6.77; 95% CI, 1.50 to 30.53; P=0.013) on computed tomography taken at Day 1. Infarct volume of >210 mL predicted malignant progression with 56.3% sensitivity and 90.9% specificity. Among the malignant progressors, 77.7% resulted in grave outcomes even with DHC, while all patients who declined surgery died.
Conclusion
Acute ischemic stroke patients with malignant cores between 82 to 209 mL can be primarily treated with neurocritical care based on reperfusion and hypothermia with feasible results. In patients undergoing surgical decompression due to malignant progression, the functional outcomes were not satisfactory.
INTRODUCTION
The combined analyses of decompressive hemicraniectomy (DHC) trials have shown that in patients with malignant middle cerebral artery (MCA) infarction, DHC undertaken within 48 hours of stroke onset reduces mortality and increases the number of patients with a favorable functional outcome [1]. However, since the success of DHC trials, there have been radical changes in the field of acute stroke. In terms of reperfusion, intravenous (IV) thrombolysis has been approved for the time window of up to 4.5 hours [2], and endovascular treatment (EVT) has become the standard of care [3]. Neurocritical care for patients with massive ischemic stroke has also improved, especially in terms of neuroprotection and the antiswelling effect of therapeutic hypothermia [4]. While the therapeutic benefits of hypothermia on functional outcomes need to be further validated in prospective trials [5], there is evidence that it can reduce cerebral edema, reduce hemorrhagic transformation and improve outcomes, especially in those with complete reperfusion [4,6]. These developments have possibly increased the number of patients eligible for reperfusion therapies, while potentially reducing the number of patients that show malignant progression [7].
Furthermore, in acute stroke populations eligible for reperfusion, DHC trials could not be applied, as randomization usually occurred at least 12 hours after symptoms onset [8], and usually did not include patients in the acute period who underwent IV thrombolysis [9]. Accordingly, there are currently few indicators for the optimal management of acute stroke patients with large vessel occlusion presenting with malignant infarct cores.
For such patients, our institution pursues rapid reperfusion, combined with primary neurocritical care based on therapeutic hypothermia. The impact of malignant progression and its predictive factors have not been studied in this population. Furthermore, the outcomes of emergent DHC in patients primarily managed with neurocritical care have not been reported. Therefore, the aim of our study was to address these points.
METHODS
Patient enrollment
This was a retrospective single center study from January 2010 to March 2015. In this period, 315 patients underwent our institutional stroke endovascular reperfusion critical pathway. Of these patients, those with acute ischemic stroke involving the MCA territory with infarct volume >82 mL on baseline diffusion weighted image (DWI) who presented within 6 hours from onset [10], with National Institutes of Health Stroke Scale (NIHSS) ≥15 (according to previous literature that malignant cerebral edema is seldom encountered in patients with NIHSS under 15) [11] were included. Infarct size was measured in baseline DWI using nordicICE semiautomated software (NordicNeuroLab, Bergen, Norway). Patients with significant contralateral infarction or space occupying intrainfarct hemorrhage were excluded.
The data collection protocol was approved by the Institutional Review Board of each participating hospital and implemented in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments. The need for written informed consent was waived given the retrospective nature of the study.
Reperfusion treatment
IV thrombolysis and endovascular reperfusion treatment were performed on patients based on the decision of the attending stroke neurologist. All patients underwent cerebral angiography for the initial intent of mechanical thrombectomy. In patients with very large DWI infarct volumes, aggressive reperfusion was avoided after performing digital subtraction angiography. However, as most of the patients were managed before the success of major EVT trials, and there is still disagreement about the upper infarct volume limit for EVT, reperfusion was sometimes performed for very large infarcts.
Primary neurocritical care
All patients were managed with intent for primary neurocritical care. This was performed based on a stepwise protocol, and the treatment degree was individualized on a patient by patient basis [12]. In brief, the treatment starts with general management including head elevation, easy venous drainage, and avoidance of fever, hypoxia, hypercapnia, or hyponatremia. Early rapid sequence intubation was performed on patients with altered mental status, or those in which therapeutic hypothermia was performed. In patients who underwent hypothermia, cooling was performed with adequate sedation and neuromuscular blockade. Patients underwent 48 hours of cooling (target temperature 34.5°C) and 48 hours of rewarming. Osmotherapy was performed with mannitol or hypertonic saline as required.
Malignant progression and DHC
Late DHC was usually performed based on clinical signs. Throughout neurocritical care, clinical signs of progressive herniation such as significant decrease in mentality, unilateral pupillary abnormality, impairment of eye movements, respiratory pattern abnormalities, and flexor or extensor motor posturing [13] were screened. Patients that showed these clinical signs, with computed tomography (CT) evidence of impending or imminent herniation, were termed as malignant progressors. DHC was performed on these patients as soon as possible after clinical decision and consent. There were no age limitations for decompressive surgery if family agreement was obtained. Previous IV thrombolysis was not a contraindication for decompression in this study. It was not performed on patients with bilateral fixed pupils [1].
Statistical analysis
First, the patients were dichotomized to malignant progressors and nonprogressors. Factors predictive of malignant progression were evaluated through univariate and multivariate analysis. Second, the impact of initial DWI volume on prediction of malignant change was evaluated through receiver operating characteristic analysis. The functional outcomes of DHC performed on malignant progression were evaluated. A grave outcome was defined as a modified Rankin Scale (mRS) of 5–6. Third, factors predictive of grave outcomes in the patients that were managed with primary neurocritical care were evaluated through univariate and multivariate analysis. The data are presented as the mean±standard deviation or as the median (interquartile range). A P<0.05 was considered statistically significant. For multivariate analysis, variables with P values <0.100 were included for logistic regression analysis by the forward conditional method. Statistical analyses were performed using IBM SPSS Statistics software version 25 (IBM Corp., Armonk, NY, USA).
RESULTS
Overall outcomes
A total of 49 patients were included for analysis in this study. IV thrombolysis was performed in 37 patients (75.5%) and EVT was performed in 39 patients (79.6%). Any form of reperfusion was performed in 45 patients (91.8%), while both IV thrombolysis and EVT was performed in 31 patients (63.3%). Therapeutic hypothermia was performed in 27 patients (55.1%). Among the 49 patients, 33 (67.3%) could be managed with primary neurocritical care, without malignant progression. In the nonprogressors, 3-month functional outcomes of mRS 0–3 were achieved in 27.3%, while grave outcomes were recorded in 42.4%. However, among the malignant progressors, 87.5% resulted in grave outcomes (Table 1).

Factors predictive of malignant progression
Prediction of malignant changes
In the analysis to detect potential factors predictive of malignant progression, initial DWI lesion volume (odds ratio [OR], 1.01; 95% confidence interval [CI], 1.00 to 1.02; P=0.046) and parenchymal hematoma, postprocedure or at Day 1, by CT (OR, 6.77; 95% CI, 1.50 to 30.53; P=0.013) showed significant association, highlighting the impact of initial infarct volume on malignant progression (Table 1). EVT, or IV osmotherapy with mannitol, was associated with malignant progression in the univariate analysis, but this association was not apparent in the multivariate analysis.
When the predictive ability of initial DWI for malignant progression was assessed, it could predict malignant course with an area under the curve of 0.735 (range, 0.569 to 0.901) (Fig. 1). Infarct volume of >210 mL predicted malignant progression with 56.3% sensitivity and 90.9% specificity. When the included patients were divided into subgroups according to initial infarct volume, the percentage of malignant progressors increased sharply when the infarct volume increased to >210 mL, with 42.9% progressors in the 201 to 299 mL group, while all patients with >300 mL of infarct core showed malignant progression (Fig. 1).

Distribution of initial diffusion weighted imaging (DWI) volumes and receiver operating characteristic (ROC) curve in prediction of malignant change. (A) The percentage of patients with malignant progression sharply increases with initial DWI volumes of >210 mL. (B) For prediction of malignant progression with initial infarct volume, the area under the ROC curve is 0.735, and an infarct volume threshold of >210 mL predicted malignant progression with 56.3% sensitivity and 90.9% specificity. AUC, area under the curve.
Impact of decompressive surgery
Among the 16 malignant progressors, nine underwent DHC and seven refused surgery. In the nonprogressors, grave outcomes were encountered in 42.4% of patients. However, of the malignant progressors, 87.6% resulted in grave outcomes (P=0.031) (Fig. 2). Even with DHC, 77.7% resulted in grave outcomes, while all patients that declined surgery died.

Functional outcomes of nonprogressors and malignant progressors. DHC, decompressive hemicraniectomy; mRS, modified Rankin Scale.
Outcomes in the nonprogression group
When the factors predictive of grave outcomes in the nonprogressors were delineated, age (OR, 1.08; 95% CI, 1.01 to 1.16; P=0.024) and initial DWI volume (OR, 1.03; 95% CI, 1.00 to 1.05; P=0.049) were shown to be significant predictive factors (Table 2). Performing EVT was associated with mRS 0–4 in the univariate analysis, but this association was insignificant in the multivariate analysis. There was a tendency for therapeutic hypothermia, resulting in more frequent mRS 0–4 (P=0.062).
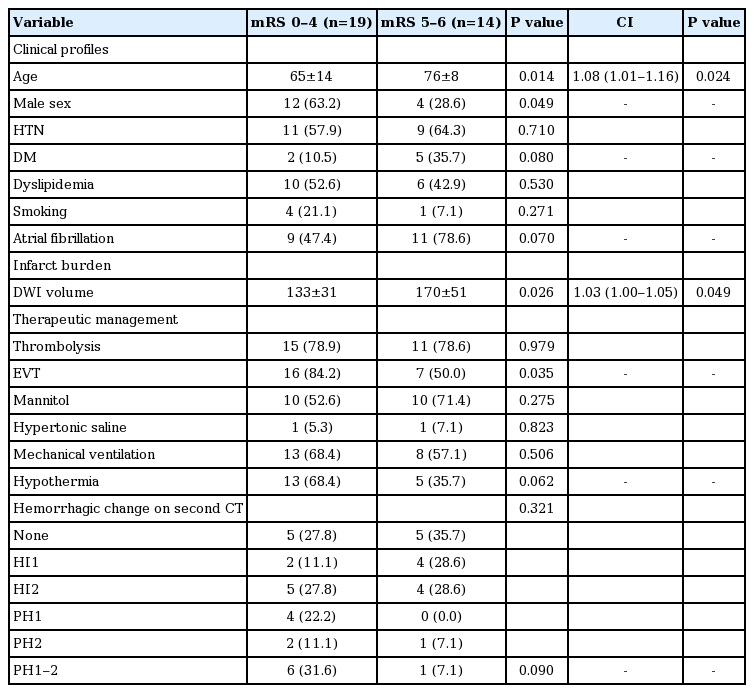
Factors predictive of outcomes in the nonprogressors
DISCUSSION
The results of this study show that primary neurocritical care with reperfusion and therapeutic hypothermia is feasible for acute ischemic stroke with malignant infarct cores. Factors predictive of malignant transformation are presenting infarct volume and occurrence of parenchymal hematoma. An infarct volume >210 mL was associated with increased ratios for malignant course. For those patients in which malignant progression occurred, decompressive surgery did not seem to offer much benefit for improved functional outcomes, most likely due to the large infarct burden.
The primary finding of this study shows that in this population, malignant progression was a major determinant of functional outcomes. As previously reported, initial infarct volume [14] and parenchymal hematoma type hemorrhages [15] were strong predictors of malignant change also in this population. In contrast, endovascular reperfusion or thrombolysis was not significantly associated, showing that potential reperfusion injuries are mostly influenced by the burden of initial infarct volume.
In the malignant progressors, however, DHC did not result in the robust functional improvements seen in the DHC trials1 that showed 78% survival and 43% with mRS ≤3. This finding may be explained in two ways. First, due to the large infarct volumes (despite earlier presentations), the patients included in this study may have shown more fulminant course than those included in the decompressive craniectomy trials. This is evidenced by the concept of late window paradox [16], in which a larger core at presentation can suggest rapid growth with poor collaterals [17] or complex type occlusions [18]. Second, the patients that would have obtained functional benefit with decompressive craniectomy could have been tolerably managed with primary neurocritical care. As a result, only the patients with fulminant infarcts may have been selected for DHC and such bias could have caused the dismal outcomes in the decompressive surgery group. If this is the case, the effectiveness of reperfusion and neurocritical care on patient outcomes may diminish the potential benefits of decompressive surgery in actual clinical practice.
The findings of our study also potentially extend the volume threshold for reperfusion therapy. As compared to patients with initial infarct volume in the 82 to 144 mL range, patients with infarct volumes in the 145 to 209 mL range did not show an increased chance of malignant progression. This is in contrast to the selection criteria of infarct volumes >145 mL that was used for the decompressive surgery trials [8]. Furthermore, when considering that the patients analyzed in this study presented earlier with evolving infarcts, the same 145 mL cut-off would include patients with potentially more malignant profiles. Thus, we can postulate that a large number of patients considered for decompressive surgery previously would have been manageable with a combination of reperfusion treatment and neurocritical care. The upper infarct volume limit of EVT has not been clearly defined and numerous studies have tried to extend the limit, which was previously taken to be an Alberta Stroke Program Early CT Score (ASPECTS) score of 6 [19]. In such studies, EVT was shown to reduce infarct growth, reduce the need for hemicraniectomy and improve outcomes in patients with ASPECTS of 5 to 7 [20]. Another study suggested a final infarct volume threshold of 133 mL as a cut-off for unfavorable outcomes after EVT [21]. Our study data further suggest that through the use of reperfusion therapy combined with primary neurocritical care, initial infarct volumes between 145 to 209 mL can be potentially manageable. Such findings warrant future prospective trials.
Our study has some limitations. First, it is limited by the retrospective nature of the study and number of patients. However, malignant cerebral edema is a rare disease with an incidence of 10 to 20 per 100,000 per year [22], and acute ischemic stroke with malignant core occurs even less often. Thus we believe that our study findings well describe the clinical characteristics and outcomes in this special population, that will gain more clinical attention, as indications for EVT expand. In this context, future studies are needed to validate these findings. Second, the study included patient data from 2010 to 2014. During this period, financial reimbursement for stent retrievers was not permitted and second generation direct aspiration devices were not yet introduced [23]. Thus, outcomes of EVT were somewhat below current standards and this should be taken into account when interpreting the results of this study.
In conclusion, acute ischemic stroke patients with malignant cores between 82 to 209 mL can be treated with primary neurocritical care based on reperfusion and therapeutic hypothermia, with feasible results. In patients undergoing emergent surgical decompression due to malignant course, the functional outcomes were not satisfactory.
Notes
Conflict of interest
No potential conflict of interest relevant to this article.
Author contributions
Conceptualization: DL, JL, HY, CE. Data curation: DL, JL. Formal analysis: HY. Funding acquisition: not applicable. Methodology: DL, JL. HY, CE. Project administration: DL, JL. Visualization: DL, JL, HY. Writing—original draft: DL. Writing—review & editing: DL, JL, HY, CE.