INTRODUCTION
Miliary tuberculosis (TB) is a rare form of TB, and data from the US Centers for Disease Control and Prevention in 2012 indicated that approximately 3.5% of all cases of TB were classified as miliary TB [1]. Furthermore, miliary TB can occur on the background of a previous malignancy, but also mimics metastatic cancer [2,3]. Here, we report an interesting case of miliary TB mimicking brain metastasis from renal cell carcinoma.
CASE REPORT
A 72-year-old woman was referred to the neurosurgery department of our hospital because of abnormal findings on a brain computed tomography (CT). She had been healthy until two month before. Recently, the patient presents complaining of several weeks of generalized weakness and poor oral intake, when dysarthria and sluggish speech developed. She was a nonsmoker and denied using illicit drugs or other relevant medical history. She had no family history of TB and denied a contact with a person with TB infection. On examination, she appeared well: body weight, 54 kg; height, 160 cm; temperature, 36.5°C; blood pressure, 140/80 mmHg; pulse, 78 beats/min; respiration rate, 20/min; oxygen saturation, 99% while breathing ambient air. The remainder of the examination was normal, including the neurologic examination. Laboratory results were normal. A human immunodeficiency virus (HIV) antibody test was negative.
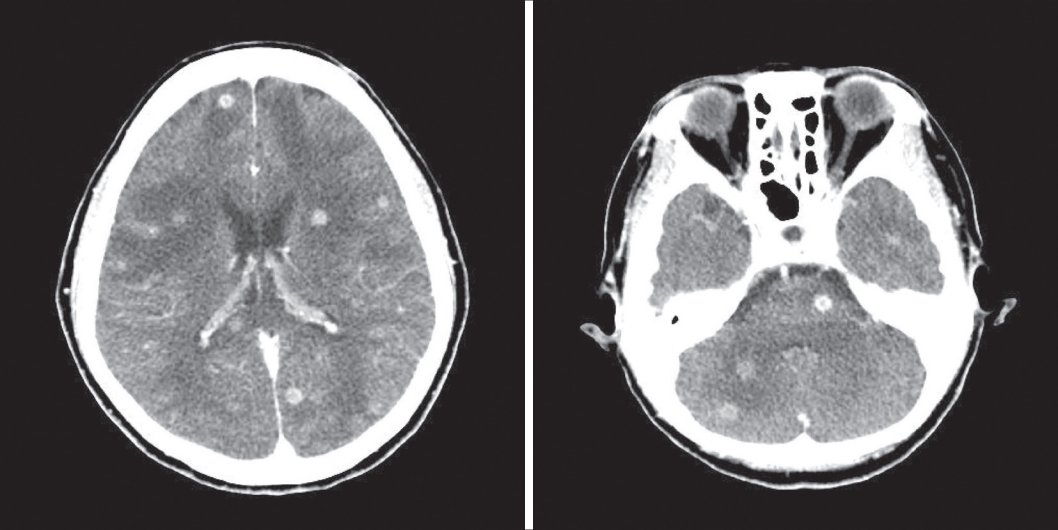
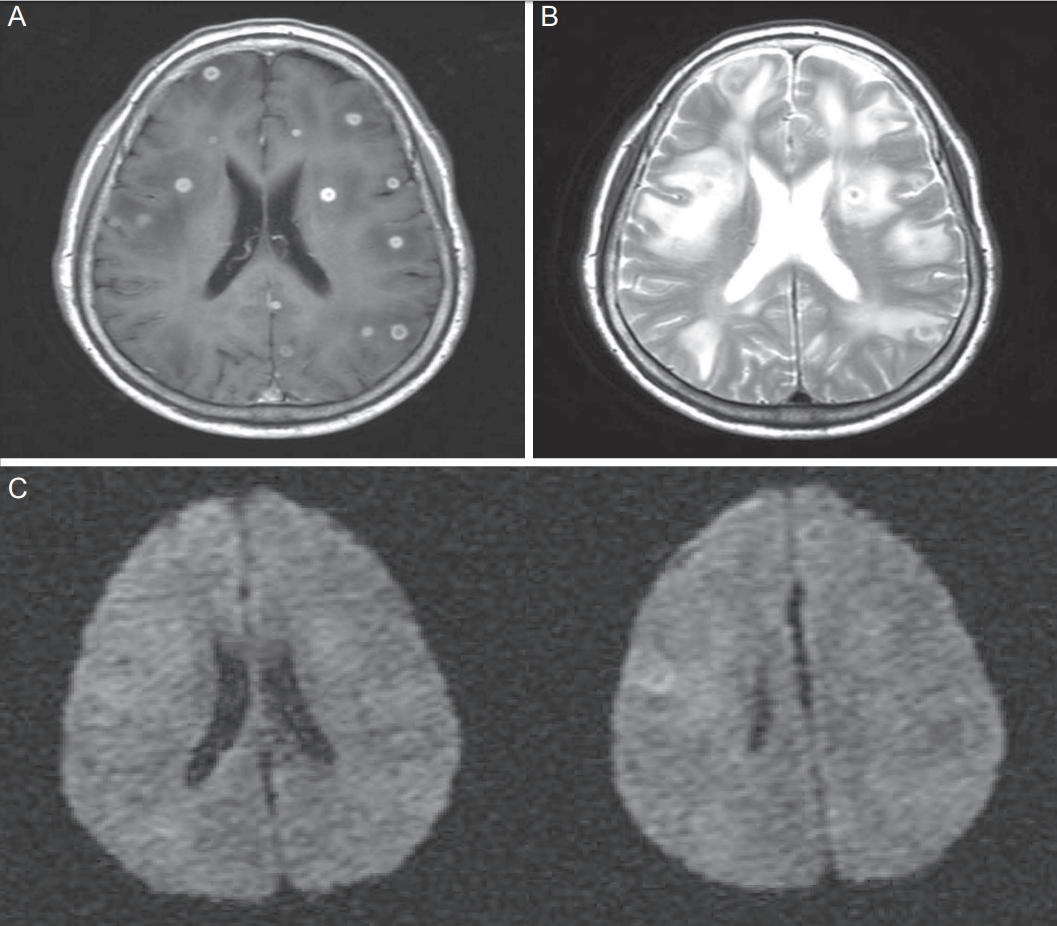
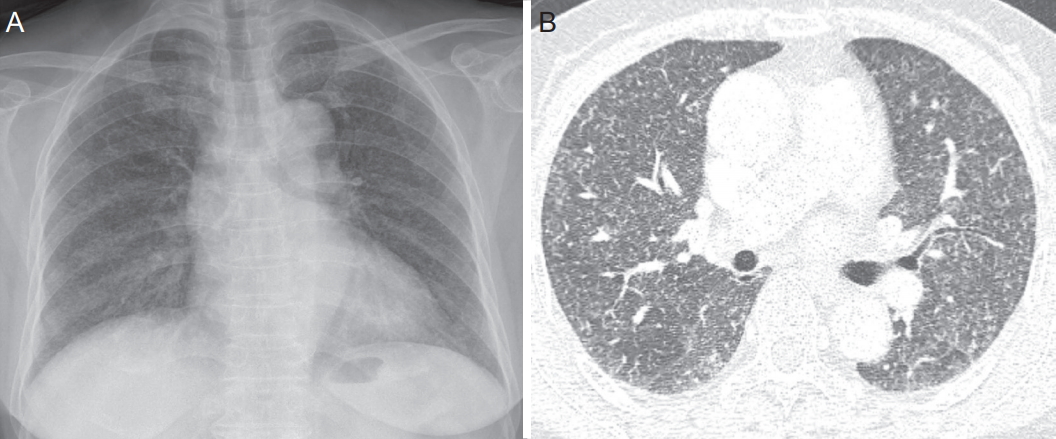
A CT scan of the head, obtained after the administration of contrast material (Fig. 1) outside hospital, showed numerous small enhancing nodules with marked edema in both cerebral and cerebellar hemispheres and the brain stem. Next, brain magnetic resonance imaging (MRI) was performed. Axial T1- and T2-weighted contrast-enhanced MRI confirmed the results of the CT (Fig. 2A, B). Also, some abnormal restricted lesions were seen in diffusion-weighted imaging (Fig. 2C). A chest radiograph and a CT scan of the chest revealed uniform-sized small nodules randomly distributed throughout both lungs (Fig. 3). A lumbar puncture was performed. Cerebrospinal fluid analysis showed: opening pressure 125 mmH2O; color clear; pH 8.0; white blood cells negative; protein 33.7 mg/dL (normal, 10-50); glucose 81 mg/dL (blood glucose 122 mg/dL); and adenosine deaminase 1.2 IU/L. Queckenstedt test demonstrated free cerebrospinal fluid (CSF) communication. CSF Gram, acid-fast bacilli (AFB) and India ink stains were negative. Mycobacterium tuberculosis polymerase chain reaction (PCR) produced negative results. Initial sputum AFB was negative. An abdominal CT scan with contrast enhancement showed an ill-defined delayed-enhancing mass-like lesion involving the right lower kidney (Fig. 4A). Wholebody positron emission tomography/CT scan showed a diffuse, intensely hypermetabolic mass in the right kidney (Fig. 4B). A diagnosis of metastatic renal cell carcinoma was made, and the patient received two doses of radiotherapy for the purpose of reducing her neurologic symptoms, without improvement.
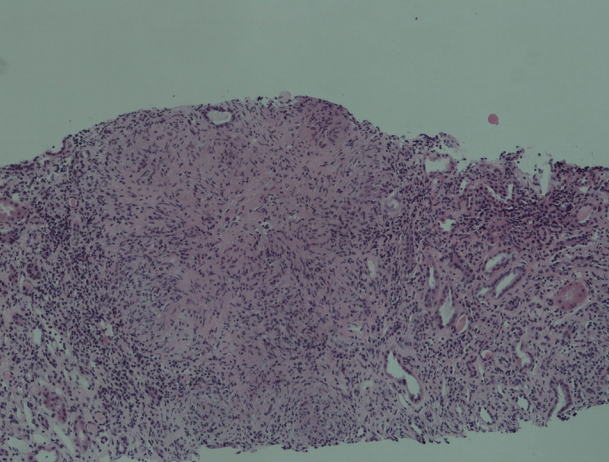
We performed bronchoalveolar lavage (BAL) and transbronchial lung biopsy (TBLB) at the anterior segment of the right upper lung. The next day, the microbiological investigation of BAL fluid by TB PCR gave a positive result, but there was no evidence of TB infection in the TBLB specimen. We therefore diagnosed the patient with miliary TB. One week after she visited the emergency room, she was treated with isoniazid, rifampicin, ethambutol, and pyrazinamide. She received intravenous dexamethasone 0.4 mg/kg per day and then tapered off. For the differential diagnosis of renal cell carcinoma, a renal biopsy was performed. The histopathological findings demonstrated chronic granulomatous inflammation with positive TB PCR, but acid-fast bacilli staining was negative (Fig. 5). Her symptoms began to improve one week after she received the anti-TB agents and she was discharged without complications.
Four weeks later, the patient returned to the hospital because of relapse of dysarthria and intermittent disorientation. The follow-up brain MRI showed no gross intervening changes in the numerous small rim-enhancing nodules and several new lesions had developed (Fig. 6A). To confirm that the diagnosis was accurate, a stereotactic brain biopsy was performed, but only reactive astrocytosis was observed, with negative results in TB PCR. Therefore, it was suggested that the patient be diagnosed with a paradoxical response, and corticosteroid was added to the treatment. After treatment for two more weeks, the patient’s neurologic symptoms had improved. Mycobacterium tuberculosis was isolated from the BAL fluid and a solid media drug sensitivity test revealed no resistance to any anti-TB agent. A follow-up brain MRI after three months showed that both the multiple intracranial nodules and the surrounding edema had nearly disappeared (Fig. 6B). Finally, the patient was diagnosed with miliary TB associated with multiple intracranial tuberculoma with a subsequent paradoxical response to anti-TB therapy.
DISCUSSION
Although the World Health Organization Stop TB Strategy has helped to reduce the overall incidence of TB since 2004, TB remains a challenging problem in several countries, including developing countries such as South Korea. Miliary TB is considered to be extrapulmonary TB in the past, but classified as pulmonary TB because there are lesions in the lungs despite the multiplicity of organs affected. Because of its characteristic of multiorgan involvement, miliary TB can be a potentially lethal disease if it is not diagnosed and treated early [2,3].
Although miliary TB has recently occurred more commonly in older than in younger people, in the past it occurred mainly in children [3]. It appears to be a result of endogenous reactivation of TB and a consequent massive lymphogenous and hematogenous dissemination [3], and the widespread use of immunosuppressive, immunomodulating, and cytotoxic agents to treat various conditions in older people may be one reason for the shift in age-specific incidence. This shift can cause diagnostic confusion for clinicians because the radiological appearance of miliary TB can resemble that of metastatic cancer; there have been several reports that miliary TB mimics metastatic cancer [2,4]. Furthermore, the efficacy of microbiological confirmation of miliary TB is unsatisfactory compared with that for pulmonary TB, despite the fact that miliary TB nearly always involves the lungs. It is known that only 30% to 65% of cases of miliary TB are positively diagnosed on the basis of culture of the pathogen from sputum [5]. Bronchoscopic examination with combinations of BAL and TBLB would be expected to have a higher diagnostic yield [6].
In our case, the patient was initially suggested, based on the radiological images, to have renal cell carcinoma with multiple metastases to lung and brain. However, the additional diagnostic approaches of BAL, TBLB, and renal biopsy revealed TB infection involving multiple organs, rather than a malignancy. As a result, our patient was finally diagnosed with miliary TB mimicking brain metastasis from renal cell carcinoma. The patient improved after a relatively short duration of anti-TB treatment. However, her neurologic symptoms unfortunately worsened, and follow-up brain MRI suggested the possibility of the concurrent existence of miliary TB and brain tumor. An additional diagnostic procedure of brain biopsy revealed no evidence of malignancy. Therefore, we concluded that the patient should be diagnosed with miliary TB with a subsequent paradoxical response to treatment, and continued with the anti-TB medication. The paradoxically enlarged intracranial tuberculomas had nearly resolved in the follow-up brain MRI.
A paradoxical response is defined as the clinical or radiological worsening of preexisting TB lesions or the development of new lesions not attributable to the normal course of disease, in a patient who initially improved with anti-TB therapy [7]. A paradoxical response can occur in 10% to 15% of TB patients who do not have concurrent HIV infection [8]. The immunological components involved in a paradoxical response have not been fully described, but some studies suggest that it may be mediated by an exaggerated response to the release of mycobacterial antigen from dying organisms [8,9]. One study suggested that patients whose treatment is complicated by a paradoxical response are more likely to have lower baseline lymphocyte counts, followed by a surge [9]. However, unlike this previous report, our patient did not have relatively low baseline lymphocyte counts followed by a surge. In a recent prospective cohort study, predictors of paradoxical reaction were female gender, HIV positivity and a shorter duration of illness [10]. Since our patient was female and had relatively short-duration of illness, these are considered to be consistent with previous findings. To reduce the paradoxical reaction, corticosteroid regimen consisted of intravenous dexamethasone for 4 weeks (0.4 mg/kg/day and then tapered off decreasing 0.1 mg/kg every week) and then oral treatment for 4 weeks, starting at a total of 4 mg per day and decreasing by 1 mg each week [10].
A large number of infectious and non-infectious diseases can cause multiple brain enhancing lesions. In one prospective Indian study, TB was the commonest infective pathology, followed by neurocysticercosis. Neoplastic diseases were common non-infective causes [11]. Therefore, it is important to distinguish TB granuloma from brain metastasis. MRI is generally considered to be superior to CT scan in assessing central nervous system (CNS) TB, and has been used in the diagnosis [12]. However, CNS TB of MRI feature is sometimes non-specific, because it has other radiologic manifestation either diffuse form as basal exudative leptomeningitis or in a localized form as tuberculoma, abscess, or cerebritis [12]. So, it may mimic other infectious or non-infectious etiology such as metastatic tumor. In our case, MR imaging of the brain showed multiple ring-enhacing nodules. In an attempt of differential diagnosis of multiple ring-enhacing nodules, Garg and Sinha [11], described some aspect of MRI feature (Table 1).
Although acid-fast staining of CSF is the most rapid method for detection of mycobacteria, this lacks sensitivity. Isolation of Mycobacterium tuberculosis from CSF can be insensitive if large amounts of CSF (≥2 mL) are not tested [13]. In addition, although PCR has been reported to be relatively specific in most reports (82-100%), its sensitivity has ranged from 32% to 100% [14]. To distinguish miliary brain TB from brain metastasis, proton magnetic resonance spectroscopy (MRS) may also serve as a diagnostic tool. Neoplastic lesions have elevated Cho, decreased Cr and NAA, while non-neoplastic lesions such as cerebral ischemia and cerebral abscesses had markedly decreased in Cho, Cr, and NAA. Furthermore, lipids and lactate are normally not detectable in a healthy brain. The lipids detected by MRS reflect the degree of micro- and macronecrosis. The intracranial metastatic tumor showed relatively higher lipid levels than what is reflected in a non-metastatic brain tumor. However, in case of TB abscess or toxoplasmosis, this method has a limited application [15].
In conclusion, clinicians should be aware that miliary TB, despite its rarity, can mimic metastatic cancer even in older people, especially in TB-endemic regions such as Korea. In addition, the possibility of a paradoxical response should also be suspected in patients who present with new neurological findings while on anti-TB therapy, because the occurrence of a paradoxical response is not uncommon.