Extremely elevated international normalized ratio in a patient using dabigatran etexilate: a case report
Article information

Abstract
Background
We present the case of a patient who was administered dabigatran and showed an extremely elevated prothrombin time-international normalized ratio (PT-INR).
Case report
A 79-year-old man was referred due to PT-INR 12.6. The patient was taking 110 mg of dabigatran twice daily in capsule form. On admission, blood urea nitrogen level was 23 mg/dL, creatinine was 1.51 mg/dL, and the estimated glomerular filtration rate was 44.8 mL/min/1.73 m2. Coagulation tests revealed PT 96.8 seconds, PT-INR 12.46, and activated partial thromboplastin time 125.5 seconds. Dabigatran was discontinued, PT-INR on the day after admission was 8.96. PT-INR recovered to 1.61 on the fourth day without any treatment.
Conclusion
The PT-INR was not directly correlated with dabigatran activity. Regular monitoring of coagulation was not necessary in all patients taking dabigatran. However, it may be useful to regularly perform coagulation tests in patients with renal impairment or in those at a high risk of bleeding.
INTRODUCTION
In general, blood coagulation tests are not necessary in patients using non-vitamin K-dependent oral anticoagulants (NOACs) [1,2]. If the patient follows the prescribed indications for NOACs, adjusting the dosage or administration interval of the medication according to the changes in coagulation tests is not necessary [3]. Here, we present the case of a patient with nonvalvular atrial fibrillation (NVAF) who was taking dabigatran and showed an extremely elevated prothrombin time-international normalized ratio (PT-INR).
CASE REPORT
A 79-year-old man living in a nursing home visited the primary hospital with fever and an oxygen saturation level of 70%. Chest computed tomography findings were suggestive of pneumonia, and laboratory findings revealed PT-INR 12.6. The patient was transferred to our hospital with cerebral infarction, persistent NVAF, congestive heart failure, dementia, benign prostatic hyperplasia, and hypothyroidism. At admission, his vital signs were as follows: blood pressure 110/73 mm Hg, heart rate 93/min, oxygen saturation 98%, and body temperature 36.3 ℃. The physical examination results were normal. There were no focal neurological abnormalities, except for decreased memory function. The patient was on the following medications: levothyroxine sodium, furosemide, spironolactone, isosorbide dinitrate, atorvastatin, donepezil, tamsulosin, and dabigatran 110 mg twice daily in capsule form without a nasogastric tube.
Blood tests in emergency room revealed a hemoglobin level of 13.3 g/dL, hematocrit 39.7%, white blood cell count 19,680/mm3, platelet count 161,000/μL and C-reactive protein 2.9 mg/dL (Table 1). Blood urea nitrogen (BUN) was 23 mg/dL (normal range, 7–25 mg/dL), serum creatinine (Cr) was 1.51 mg/dL (normal range, 0.5–1.2 mg/dL), and estimated glomerular filtration rate (eGFR) was 44.8 mL/min/1.73 m2. Coagulation tests showed that PT was 96.8 seconds (normal range, 11–15 seconds), PT-INR was 12.46 (normal range, 0.8–1.2), and activated partial thromboplastin time (aPTT) was 125.5 seconds (normal range, 28–45 seconds), which were exceptionally increased. Thrombin time (TT) could not be measured because clot formation did not occur, and ecarin clotting time (ECT) could not be performed. Serum albumin levels and liver function test results were normal. Blood tests performed three months prior showed BUN 14.7 mg/dL, Cr 0.93 mg/dL, and eGFR 78.4 mL/min/1.73 m2. PT and aPTT were not measured at that time. Comparison with the previous laboratory results revealed a rapid decline in renal function during this visit. No signs of sepsis or liver dysfunction were observed, and a patchy opacity was observed in the left lower lobe on chest radiography, suggesting pneumonia. Piperacillin-tazobactam intravenous (IV) injection was initiated.
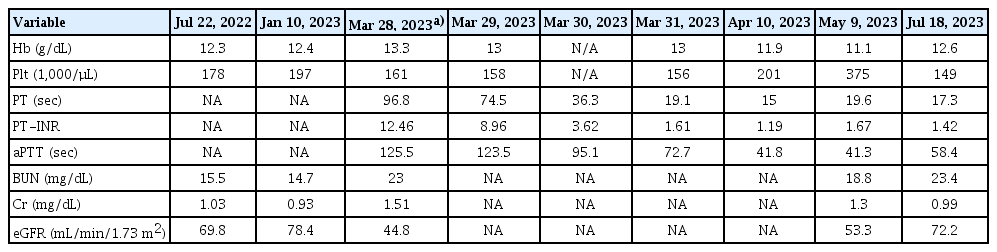
Serial changes in blood coagulation and kidney function tests during the treatment
Although coagulation tests revealed abnormalities, no bleeding-related symptoms or signs were observed. Therefore, vitamin K and fresh frozen plasma were not used, and dabigatran was discontinued. Idarucizumab was not administered because it was unavailable at our hospital. The patient remained clinically stable, and the PT-INR measurement conducted on the day following admission yielded a result of 8.96. PT-INR recovered to 1.61 on the fourth day without any special treatment. The patient was discharged with an oral administration of 100 mg aspirin instead of dabigatran. Fourteen weeks later, blood tests showed PT 17.3 seconds, PT-INR 1.42, aPTT 58.4 seconds, BUN 23.4 mg/dL, Cr 0.99 mg/dL, eGFR 72.2 mL/min/1.73 m2, and there were no bleeding-related symptoms.
DISCUSSION
NOACs are primarily used to prevent ischemic stroke or transient ischemic attacks in patients with NVAF. Currently, dabigatran, rivaroxaban, apixaban, and edoxaban are available [4]. Among them, dabigatran was the first NOAC approved for stroke prevention in patients with NVAF and acts as a direct thrombin inhibitor. Thrombin is a multifunctional enzyme that converts fibrinogen to fibrin and activates platelets. Dabigatran etexilate is the prodrug of dabigatran, a potent, nonpeptidic small molecule that specifically and reversibly inhibits both free and clot-bound thrombin by binding to the active site of the thrombin molecule [5]. It competitively inhibits thrombin in a concentration-dependent manner.
Dabigatran etexilate has a mean absolute bioavailability of 6.5%, which is independent of the dose and is not influenced by co-administration with food. It is present in capsules containing multiple pellets with a tartaric acid core to facilitate gastrointestinal absorption. This generated an acidic environment that favored drug dissolution and absorption. After oral administration, dabigatran etexilate is rapidly hydrolyzed to its active form by ubiquitous esterases. Given that cytochrome P450 enzymes and other oxidoreductases are not involved in the proteolytic reactions that convert dabigatran etexilate to dabigatran, the risk of drug-drug interactions is low.
Peak plasma concentrations (Cmax) and anticoagulant effects are achieved within 1.5 to 3 hours after oral dosing. Plasma concentrations show biphasic decline. The first phase is characterized by a rapid distribution phase. This is followed by a prolonged terminal elimination phase, resulting in a mean plasma terminal half-life of 12–14 hours, independent of the dose. Consequently, therapeutic concentrations are maintained for 24-hour periods, while retaining sufficient reversibility. The renal excretion of unchanged dabigatran is the predominant elimination pathway, with approximately 80% of the IV dose excreted unchanged in the urine. The remainder is conjugated with glucuronic acid to form acyl glucuronides, which are predominantly excreted via bile, with only very small amounts of conjugates found in urine.
In our patient, there were no bleeding symptoms during dabigatran administration; however, an exceptional abnormality in the coagulation tests was observed. To date, no laboratory studies are available to confirm dabigatran-induced coagulopathy in a general hospital setting. The most sensitive clotting assays were the TT and ECT, followed by the aPTT and PT-INR. Normally, the PT-INR is not directly correlated with dabigatran activity. Several conditions can induce abnormalities in coagulation test results during dabigatran use. First, kidneys play a major role in NOAC excretion. Approximately 80% of dabigatran is excreted by the kidneys, and dosage adjustments should be considered based on renal function [6,7]. According to the Korean Arrhythmia Society guidelines, for patients with a creatinine clearance rate of 30–50 mL/min, dabigatran administered twice daily at a dose of 110 mg is recommended [8]. In our case, the eGFR value at the time of admission was 44.8 mL/min/1.73 m2 compared to 78.4 mL/min/1.73 m2 three months ago, indicating progressive renal failure. However, he was taking 110 mg of dabigatran twice daily before admission and did not overdose. Second, while our patient took all medications without crushing them into powder form, it is not recommended to remove capsules before administration because it increases the bioavailability of dabigatran by more than 75%, and powerful P-glycoprotein inhibitors can increase NOAC plasma concentrations owing to drug interactions related to dabigatran. However, no relevant drugs were administered. Despite extensive literature reviews, the exact mechanisms underlying the extremely elevated coagulation test results in our patient could not be explained. Only a few cases have reported that PT-INR decreased after management with idarucizumab, suggesting a possible relationship between dabigatran use and PT-INR [9,10].
Our patient showed an elevated PT-INR on the 40th day after the discontinuation of dabigatran. Although there are reports that doses of aspirin 2–3 g/day can prolong PT-INR, low-dose aspirin does not usually affect PT-INR [11]. Multiple factors can interfere with PT-INR, such as antibiotics, antifungals, chemotherapeutics, amiodarone, allopurinol, serotonin reuptake inhibitors, acute illness, chronic liver disease, coagulation homeostasis [3]. Even if there was an unidentified coagulopathy in our patient, we believe that the recruitment of similar patients may be essential to determine a safe dose of dabigatran and to monitor drug activity.
In conclusion, regular monitoring of coagulation tests, including PT and aPTT, is not necessary for all patients taking dabigatran. However, it may be useful to regularly perform blood coagulation tests in patients with renal impairment or in those at a high risk of bleeding.
Notes
Ethics statement
This study was approved by the Clinical Trial Review Committee of the Sanggye Paik Hospital (No. SGPAIK 2022-03-011). The requirement for written informed consent was waived, and the study was conducted in accordance with Good Clinical Practice guidelines and the Declaration of Helsinki.
Conflict of interest
No potential conflict of interest relevant to this article.
Author contributions
Conceptualization: all authors. Methodology: all authors. Software: SWH, JO. Validation: SWH, HJY. Formal analysis: JK, JO, SWH. Investigation: SWH, YJ, JO. Data curation: all authors. Visualization: JO. Supervision: HJY. Project administration: all authors. Writing–original draft: JK, SWH. Writing–review and editing: all authors.